
Toxic Megacolon
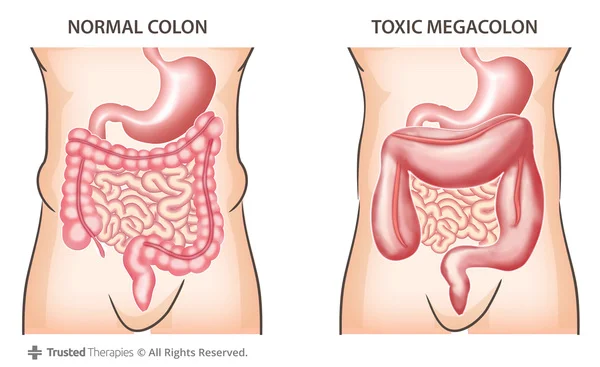
This rare gastrointestinal condition occurs when the colon (or large intestine) loses its ability to contract and has continued dilation as a result.
The gas within the colon begins to build up and causes severe abdominal distension. This distension can result in a perforation (or hole) in the intestine which allows feces to leak into the abdominal cavity. This is a life-threatening emergency and can cause widespread infection, organ failure, and death.
Causes
The actual cause of toxic megacolon is unknown. There is a higher incidence of it seen in individuals who have diseases that cause irritation to the bowel wall. These include diseases such as Crohn's Disease and ulcerative colitis. One key factor with toxic megacolon is that there is no obstruction causing the dilation.
Up to Date states that "although most commonly recognized as a complication of inflammatory bowel disease (IBD), toxic megacolon may also occur with infectious colitides of diverse etiology, ischemic colitis, volvulus, diverticulitis, and obstructive colon cancer." Certain medications including narcotics, anticholinergic agents, and antidepressants can also contribute to the disease. It can also be caused by infection within the bowels. One common aggresive bowel infection includes clostridium difficile (c. diff).
Symptoms
Symptoms include the following:
- Abdominal distension
- Abdominal pain and tenderness
- Fever
- Bloody and/or diffuse diarrhea
- Painful bowel movements
- Shock including an elevated heart rate
- Absence of bowel sounds
Diagnosis of toxic megacolon includes imaging ordered by the provider. This could include an abdominal x-ray or abdominal CT scan. A colonoscopy could also be performed to visualize the colon. Different lab tests including a complete blood count (CBC) and complete metabolic panel (CMP) may be ordered to further evaluate the patient.
Nursing Interventions For Toxic Megacolon
A nasogastric tube (NG) tube will be placed to relieve as much abdominal distension as possible. The doctor will order whether the suction will be continuous or intermittent suctioning.
Continuous IV fluids as well as blood products (depending on the blood loss of the patient) will be ordered. The patient may need to have total parenteral nutrition (TPN) depending on the severity and outcome of these interventions.
A stool sample will be taken to have cultures performed. This would be to test for an underlying infection that may be causing the disease. Antibiotics will be given if an infection is suspected.
If these treatments fail, surgery may be required. The distended portion of the intestine would be removed and then the remaining bowel would be reattached (bowel resection) together. It may be necessary to create a colostomy where the colon is attached to a hole in the abdominal wall. This allows fecal matter to be excreted into this opening rather than through the rectum. This may be either temporary or a permanent solution.





